According to statistics, heart disease and cancer are the leading causes of death in the United States. But did you know that these, as well as many other health issues, all have one thing in common? This one thing is stress and its effect on adrenal health and function.
So, besides understanding adrenal fatigue and its mechanisms, one should also know what to do to help the situation. It starts by understanding what adrenal fatigue is, what happens during a crash, how to mitigate the situation, and then how to go about your long healing process.
 Your adrenals are your body’s main stress modulators. When overwhelmed, they may become overwhelmed and unable to compensate. Adrenal fatigue may result. The condition develops over a long period, sometimes even years. Many people, however, develop adrenal fatigue due to an intense experience like the loss of a loved one, acute infection, or financial distress.
Your adrenals are your body’s main stress modulators. When overwhelmed, they may become overwhelmed and unable to compensate. Adrenal fatigue may result. The condition develops over a long period, sometimes even years. Many people, however, develop adrenal fatigue due to an intense experience like the loss of a loved one, acute infection, or financial distress.
Your adrenals’ job is to return your body to a state of normal function. This complicated process may see the rise of many unpleasant symptoms. Your hormones play a significant role in the process. Those playing a major role include cortisol, adrenaline, estrogen, and androgen. Your adrenals secrete over 50 different hormones to maintain homeostasis in the body.
Hormones secreted by the adrenals play a key role in many organs and body systems. When in a state of dysregulation, you may see various symptoms develop commonly seen as health issues. During adrenal fatigue, your body will regress into a lower state of function to conserve energy in order to heal. Its primary focus is survival. We refer to this state as an adrenal crash. This period should see you resting.
If this period of rest allows for healing, the adrenal crash and its symptoms will stop and your body will start to stabilize and finally return to its pre-cash functional state. We refer to this as the recovery phase.
The crash and recovery state together are known as the crash and recovery cycle. You may see unpleasant symptoms improve or disappear during the recovery cycle. If your body cannot recover by itself, adrenal health may suffer with adrenal failure a possible outcome. Your body, however, goes through four adrenal fatigue states before adrenal failure.
The four stages progress over time and are triggered by periodic adrenal crash and recovery cycles.
 Adrenal fatigue is a strategy employed by your body to conserve energy when the adrenals become overstressed. The more advanced the condition, the more difficult your adrenals find it to function properly. The most basic physiological state is prolonged bed rest or, in the animal kingdom, hibernation. Hibernation in animals sees their bodies expending the least amount of energy possible. The advanced stages of adrenal fatigue in humans often results in prolonged bed rest.
Adrenal fatigue is a strategy employed by your body to conserve energy when the adrenals become overstressed. The more advanced the condition, the more difficult your adrenals find it to function properly. The most basic physiological state is prolonged bed rest or, in the animal kingdom, hibernation. Hibernation in animals sees their bodies expending the least amount of energy possible. The advanced stages of adrenal fatigue in humans often results in prolonged bed rest.
Worsening adrenal fatigue accompanied by a crash sees your body wanting to return to a simpler state. This involves many organ systems, with those not required for immediate survival downgrading or turned off. Reproduction, for example, is not needed for imminent survival. You may thus see a decline in libido. Thyroid function may also slow down to conserve energy, resulting in sluggishness and a reduced basal metabolic rate. Your gastrointestinal tract may also slow down, complex foods become harder to digest and absorb, and digestive enzyme and acid release reduced. You may experience symptoms that include bloating, increased gas, and constipation.
Liver and kidney function become impaired and your body stores up toxins as a result. Fat-based metabolites become stored as fat because your body cannot eliminate them. Also, when metabolites collect in the brain due to your body’s inability to eliminate them, it may impair brain function. Examples of associated symptoms include brain fog, memory loss, and anxiety.
Metabolite accumulation in the joints and muscles may result in joint pain and inflammation.
The down-regulation of body functions continues so long as your body needs to conserve energy to survive. Further down-regulation could cause muscle degeneration and thus a loss of muscle mass. Your body can go into a catabolic state. Common symptoms include chronic fatigue and fibromyalgia.
As gastrointestinal function slows down, you may experience a reduced appetite.Those with blood sugar issues or insulin resistance are particularly vulnerable during this period. Electrolyte imbalance is common.
If the condition does not reverse, your body can go into an alarm reaction. Adrenaline is released. Too much of this hormone can further contribute to the downward spiral. Your body moves closer to a crash state.
The symptoms mentioned may seem unrelated yet the progression is logical. Their progression is your body’s way of shutting down for survival. The period is hallmarked by extreme fatigue, an irregular heart rate, compromised mental function, and high adrenaline levels with low body energy levels.
Downregulation will not stop until your body finds its equilibrium, i.e., when the energy demand matches the output. Here, your body feels able to survive and not threatened. Common medications may not work once your body reaches this state. They may even make matters worse.
The crash phase sees the body decompensate with symptoms worsening. The recovery phase sees a gradual restoration of pre-crash level function.
The most prominent symptom during the adrenal crash phase is fatigue and lack of energy. The sum of all dysfunctional and dysregulated hormonal and metabolic pathways ultimately results in reduced energy output as the main outcome. Gauging the energy level during the crash phase therefore gives us the most accurate indication of the severity of the crash over time. No laboratory tests can quantify this objectively. The more the number and intensity of symptoms, the more severe the crash.
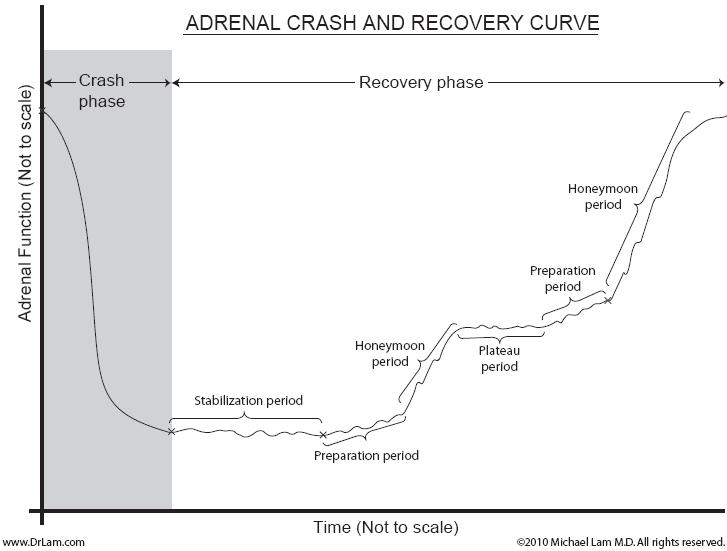
You experience a gradual return to pre-crash adrenal function and energy levels. Adrenal crash symptoms reduce and resolve and recovery proceeds. This phase is broken into a stabilization period followed by one or more mini-recovery cycles. Each consists of a preparation period, a honeymoon period, and a plateau period. The three periods flowing in sequence resembles a set of steps going up. The overall successful recovery plan consists of multiple "S" curves in an upward sustained series without any major downward crashes. This is illustrated in the graph above and is comprised of the following:
Stabilization Period: This follows the adrenal crash but occurs before the initial min-recovery leg up. The body stops decompensating and arrives at a steady state of lower function. This period plays an important role in your overall recovery phase.
Preparation Period: It can last from one day to six weeks. It depends on the stage of adrenal fatigue. The stronger adrenal function, the shorter it lasts. Your body may not feel a significant increase in energy even though you received nutrients. You may, however, feel more in control and see an improvement in mood. You may continue feeling fatigued although you may experience a subtle improvement. Your body will build lost reserves and get stronger. You may, however, experience times when you feel worse.
Honeymoon Period: This follows the preparation period and can last a few days to 12 weeks, depending on the stage of adrenal fatigue. The weaker the adrenals, the longer this period. Your body can handle stress better. Blood pressure starts to stabilize, brain fog starts to dissipate, and functional sleep returns. Mini crashes and setbacks may occur from time to time but usually last only a few days. They are more tolerable than before with a faster recovery rate. You feel better and become more optimistic.
Plateau Period: The body is stabilized. There is no set time frame for the duration of this period. It can last for weeks or months. In the early stages of Adrenal Fatigue, this phase can go on for years. You may have no symptoms during this time.
The situation is more dismal during the latter stages of adrenal fatigue. Sufferers have to slowly adapt to an overall lower level of energy function. If the adrenal function is already at its maximum, one can be stuck at this phase for a very long time without upward progress. Many self-guided programs would not be able to rise to the next cycle due to the lack of foresight and planning. This is perhaps the most trying time, as impatience sets in. Most interpret the lack of continuation and sustained improvement as failure and become disappointed. Yet many people experience a resetting time during this period where they can push their bodies into a higher level of function if taken advantage of properly.
Most Adrenal Fatigue sufferers, especially those in the advanced stages, experience multiple crash and recovery cycles. A careful analysis and comparative study of triggers and accompanying symptoms of each cycle over time serves as a good guide on overall adrenal function.
 All adrenal crashes are precipitated by a stressor event. Such events may be obvious (such as death of a loved one) or minor (such as taking a long walk). Small crashes might delude detection. It is important to fully investigate the cause of each crash. The same stressor will likely trigger subsequent crashes. This is where an expert clinician's guidance is critical. History will likely repeat itself if you do not take steps to understand the current crash trigger and take steps to prevent it from occurring again.
All adrenal crashes are precipitated by a stressor event. Such events may be obvious (such as death of a loved one) or minor (such as taking a long walk). Small crashes might delude detection. It is important to fully investigate the cause of each crash. The same stressor will likely trigger subsequent crashes. This is where an expert clinician's guidance is critical. History will likely repeat itself if you do not take steps to understand the current crash trigger and take steps to prevent it from occurring again.
Examples of situational stressors that can trigger adrenal crashes include: overwork, dehydration, long road trips, going on vacation, dental procedures, infections, overexposure to the sun, lack of sleep, sexual intercourse with ejaculation, drinking soda or coffee, medication withdrawals (especially steroids), thyroid medication sensitivity (especially T3), infections such as those resulting from flu or insect bites, overmedicating (e.g. with steroids and epinephrine),and investigative procedures such as an ACTH stimulation test. Other stress triggers include: the over-use of stimulatory supplements, metal toxicity, excessive exercise, exposure to heat such as from a sauna or steam room, exposure to toxic fumes, prolonged standing, constant anxiety, relationship difficulty, death of a loved one, a long airplane or car trip, moving to another home, overly aggressive detoxification such as enema, certain homeopathic remedies, certain massages or acupuncture, excessive improper breathing and use of stimulatory breathing exercises, and excessive stimulatory entertainment such as watching an action movie.
One should note that the more advanced the Adrenal Fatigue, the less intensity the stressor needs to be to trigger an adrenal crash. The body's reserve in advanced Adrenal Fatigue is already low and very close to hovering above the adrenal symptom threshold level. It does not take much to cross this threshold as the crash occurs.
Symptoms of adrenal crash represent a sudden intensification or abrupt onset of the many already existing pre-crash Adrenal Fatigue symptoms, such as:
You need not have all of these symptoms to have an adrenal crash. You may only have some, although often severe. The degree of decompensation may also vary between mild, major, or severe. Generally, the more intense the symptoms, the more severe the crash. You can experience any adrenal crash severity during any stage of adrenal fatigue.
 Clinically, can classify Adrenal Fatigue Crashes into 5 levels based on subjective evaluation. Levels 1 and 2 are considered minor crashes with good recovery potential. Levels 3, 4, and 5, considered major crashes, have a much less certain Recovery Phase.
Clinically, can classify Adrenal Fatigue Crashes into 5 levels based on subjective evaluation. Levels 1 and 2 are considered minor crashes with good recovery potential. Levels 3, 4, and 5, considered major crashes, have a much less certain Recovery Phase.
Level 1 - loss of 10-19% of immediate pre-crash baseline level of adrenal function in terms of energy, metabolic imbalance such as hypoglycemia, and emotional function such as irritability. You may feel more fatigued and irritable as well as hungrier than usual. Although you can carry on with normal outside and household tasks, you feel more tired at the end of the day. A nap is useful and you feel revived after resting.
Level 2 - loss of 20-29% of immediate pre-crash baseline level of function in terms of energy, metabolic imbalance such as hypoglycemia, and emotional function such as irritability. You typically experience a definite reduction in energy. A nap or thirty minute rest may compensate for this. You may see a decrease in emotional stability and become more easily irritated. Completing everyday tasks becomes more difficult although you can force yourself to complete them. You stay tired even after a nap or resting.
Level 3 - loss of 30-39% of immediate pre-crash baseline level of function in terms of energy, metabolic imbalance such as hypoglycemia, and emotional function such as irritability. Your energy levels are low throughout the day, even after taking a nap or a rest. Completing your daily tasks becomes more difficult. You want to stay at home all day. You may experience short-temperedness, anger, and rage. Sugar cravings may arise. Insomnia worsens, and is often accompanied by cold sweats, heart palpitations and dizziness.
Level 4 - loss of 40-49% of immediate pre-crash baseline level of function in terms of energy, metabolic imbalance such as hypoglycemia, and emotional function such as irritability. You may feel fatigued throughout the day. Completing your daily tasks becomes increasingly difficult. Emotions of irritability and anger may increase. Even sounds from the television set may become irritating. Once in bed, you may find it hard to get up just to go to the kitchen to prepare something to eat.
Level 5 - loss of greater than 50% of immediate pre-crash baseline level of function in terms of energy, metabolic imbalance such as hypoglycemia, and emotional function such as irritability. Bedridden most of the time, you may find yourself only able to get up to accomplish basic personal hygiene chores. It's not unusual to require assistance for ambulation, taking a shower, or changing clothes.
One can have any number of minor or major crashes during any stage of Adrenal Fatigue.
Proper crash management requires individualized attention. Everyone is different, and there are no standardized protocols. What works for one person may make another person’s symptoms worse. You need to address these issues during adrenal crash management.
This usually means a reduction in physical activities and more rest. You would need to adjust your exercise to manage the body’s energy state. In the earlier stages of Adrenal Fatigue, a crash may present itself as mild fatigue.
Exercise increases adrenaline release and blood circulation. This may cause a short-term energy boost. Unless you get enough rest after a workout, your body becomes drained, setting the scene for follow-up crashes.
Complete rest in bed is also not necessarily the solution. A personalized program of Adrenal Restorative Exercises and Adrenal Breathing Exercises may prove helpful. As the body is very sensitive to even the slightest stress, one must take care to adjust the intensity and frequency to match the body's state of adrenal health to avoid further crashes. For example, your body may not tolerate an 80 percent breathing intensity during a crash and should be adjusted down to 50 percent or less. Improper breathing techniques, such as prolonged holding, or shallow breathing, can also increase sympathetic tone and trigger further adrenal crashes.
 Hypoglycemia and metabolic imbalances may both occur during an adrenal crash. Dietary adjustments should aim at stabilizing blood sugar levels. This means balancing your carbohydrate, protein, and fat intake. An adrenal crash often affects your gastric function. Furthermore, you need to consider the way in which you get your various nutrients. For example, raw milk may prove better than regular milk or raw egg may suit your stomach better than cooked egg. Those experiencing a severe crash may not tolerate regular foods. Here, chicken broth may prove a better option, for example. Severe cases may result in hospitalization and specialized nutrition.
Hypoglycemia and metabolic imbalances may both occur during an adrenal crash. Dietary adjustments should aim at stabilizing blood sugar levels. This means balancing your carbohydrate, protein, and fat intake. An adrenal crash often affects your gastric function. Furthermore, you need to consider the way in which you get your various nutrients. For example, raw milk may prove better than regular milk or raw egg may suit your stomach better than cooked egg. Those experiencing a severe crash may not tolerate regular foods. Here, chicken broth may prove a better option, for example. Severe cases may result in hospitalization and specialized nutrition.
Salt cravings, a common symptom of Adrenal Fatigue, may result from a sodium imbalance due to hormonal dysfunction. A sodium imbalance is usually worse during a crash. One needs to take in attempting to rectify the situation. Too much sodium and low water consumption may cause hypertension and dehydration. The latter can further worsen the crash. Too much water and too little salt may cause dilutional hyponatremia.
Unfortunately, lab results may show normal during the crash and only show abnormalities once the crash has advanced. People taking diuretics or high blood pressure medications should take special care during a crash. Common symptoms associated with an electrolyte imbalance include, amongst others, nausea, vomiting, headache, malaise, and foggy thinking are common. Severe cases may need hospital admission.
You have to be careful with supplements during an adrenal crash.Certain supplements or even the same dosage of a supplement may worsen the situation during a crash. Many people, when going through an adrenal crash may have to leave off taking any supplements until the situation changes. Other people, however, may have to increase their dosage.
You should never take any nutritional supplements without first talking to your healthcare provider. Each person is different. Supplements that work for one person may not work for another. Furthermore, certain supplements may prove beneficial at different stages of adrenal fatigue. Your healthcare provider is best able to determine a supplement’s efficacy and dosage.
Signs of adrenal recovery are usually less prominent and more insidious. They include:
It is important to note that stabilization is part of the recovery process. If the adrenal symptoms do not worsen, your body is undergoing a transition from crash to recovery and then stabilization.
 The focus of recovery management is vastly different to that of the adrenal crash phase. This phase is long and can take weeks or months The weaker your body, the longer it takes. Here, we should focus on providing your body with the tools it needs to heal itself. This long journey may see you experience numerous setbacks, but healing is possible. Never push your body harder than it is unable to go during this time.
The focus of recovery management is vastly different to that of the adrenal crash phase. This phase is long and can take weeks or months The weaker your body, the longer it takes. Here, we should focus on providing your body with the tools it needs to heal itself. This long journey may see you experience numerous setbacks, but healing is possible. Never push your body harder than it is unable to go during this time.
Your body needs time to stabilize itself after dealing with a crash. The fight or flight response triggered during the crash needs to be deactivated to further set off alarm signals. To reduce the stressors on your body, you should consider making certain dietary and lifestyle adjustments. Paradoxical reactions should resolve as the stabilization period progresses.
For some unknown reason, your body may, while in the recovery phase, decide to reset and kick-start itself. It wants to return to a state it considers normal.This attempted restart may be your body’s NEM response activating its survival mechanism. This usually occurs during the plateau period during the latter stages of the stabilization period. You may experience mini crashes during this time followed by mini recovery cycles. Essentially, the attempted kick-start is your body trying to bring all systems up to a higher level of function.
These kick-start attempts do provide a beneficial function, however. Without these attempts, your body could stay in the preparation period for a long time because it is cruising and does not want to achieve better performance. These kick-starts point to your body’s natural recovery rhythm trying to support recovery.
This period may also see your body better react to the nutrients it previously chose to ignore or have reactions to. As your body utilizes them, various functions improve.
Taking the correct actions during this period may further support your adrenal glands’ return to health.
Take supplements that fit a specific purpose. You may need to make many adjustments while recovering. As your adrenal function changes, so too should the dosage. You may go through periods where you see no improvements or have periods of rest. Your body may not react to supplements as it did previously. Your healthcare provider is best able to guide you during these periods.
Enough rest is a crucial recovery factor. Be kind to yourself during crashes. These periods may see a greater need for adequate rest. Also beware of any supplements used. Those that encourage a higher energy state may take a negative toll on your body when going through a mini crash. Your body needs time to rest after each positive upswing as your body heals.
Modern medicine does not have laboratory tests that measure adrenal function throughout recuperation. Qualitative challenges are thus used to assess your progress and function. The responses to these challenges signal your adrenal glands’ reserve capacity, your tolerance to certain nutrients, and their ability to recover. Taking the right supplement dosage, the delivery system, timing, lifestyle changes, and a suitable exercise regime should be discussed with a qualified healthcare professional.
Systemic challenges means introducing certain nutrients to test the functionality of different body systems. Consuming more carbohydrates or proteins before going to bed can help discern your metabolic state during the middle of the night. Your blood sugar levels are then typically low. The response reveals your body’s ability to process glucose. This proves useful in assessing those with metabolic syndrome, insulin resistance, hypoglycemia, or sleep maintenance insomnia.
Deep breathing exercise or taking certain nutrients like tyrosine and certain herbs may help determine sympathetic nervous system function. Consuming hard to digest proteins may help in assessing gastrointestinal health. Certain supplements like magnesium DHEA, and glutathione are also valuable, especially when assessing irritable bowel syndrome.
 Further crashes can further harm your body’s state of balance. Furthermore, your body needs increasingly more energy to deal with subsequent crashes and takes longer to recover. You should do everything you can to avoid follow-up crashes. This means giving your body any additional support you possibly can to help prevent another crash and to encourage recovery. This means that, when taking supplements, the dosage should correspond to your body’s needs. A compromised body cannot properly deal with a huge influx of energy.
Further crashes can further harm your body’s state of balance. Furthermore, your body needs increasingly more energy to deal with subsequent crashes and takes longer to recover. You should do everything you can to avoid follow-up crashes. This means giving your body any additional support you possibly can to help prevent another crash and to encourage recovery. This means that, when taking supplements, the dosage should correspond to your body’s needs. A compromised body cannot properly deal with a huge influx of energy.
Besides taking types of exercise, diet, and lifestyle changes into consideration, you should have various supplements as part of your adrenal repair toolkit. Some of these may be strong and others gentle.Some have a moderating effect, while others are stimulants. Knowing how to use them and the correct dosage is paramount when it comes to adrenal support. Education, together with the help of a qualified healthcare practitioner, is key when it comes to putting together your adrenal recovery toolkit.
The following may be useful:
The dose necessary for a successful challenge varies greatly from nutrient to nutrient as well as from person to person. In the case of vitamin C, some can experience significant responses with as little as 10 mg, while others will need well over 10,000 mg. In addition to dosage, the delivery system has to be considered. Different forms of the same substrate also have different properties. Liquid forms may prove more desirable in certain situations as they allow for easier absorption into the bloodstream. Topical delivery is best for those who are highly sensitive.
Do note that where a nutrient has a negative reaction, you can always reintroduce it at a later date when your body has returned to a better state of function. Also, custom blends have a more positive effect than individual use. Individual use may cause overuse as taking a variety of nutrients could cause an overlap that increases certain reactions. This may do more harm than good. Paradoxical reactions may occur.
The length of the recovery phase depends on the individual person. The more advanced your adrenal fatigue, the longer it will take.
Recovery factor (RF) is a quantitative measurement of the Recovery Phase duration relative to crash phase duration. This helps us to appreciate the time it takes for recovery vs. the time of the crash. RF is a numerical number derived by dividing the recovery time by the crash time. If the crash duration is 1 day and the subsequent recovery duration to return to immediate pre-crash baseline is 4 days, then RF = 4/1 = 4. In other words, it takes the body four times longer to recover relative to a crash. The higher the RF number, the more depleted the adrenal reserve and the weaker the adrenal glands. RF ranges from 1-20, with the lowest number in stage 1 and the highest number in stage 4. RF gives us a rough measurement of one's adrenal function.
As Adrenal Fatigue progresses, the average RF increases. The average RF for stage 2 is 2, while the average RF for stage 3C is 7. The RF range also increases. With stage two, the RF varies from 1 to 3, or a 3 fold range. Someone in stage 3D may see a range from 6 to 30, a 5 fold increase. Those at stage 3D can expect a recovery time of 30 times or longer compared to stage 1 Adrenal Fatigue. Weaker adrenals see a wider range bias accompanied by a slower recovery rate.
Therefore, if in stage 1 of adrenal fatigue, you may spend half of the cycle in the recovery phase. As you progress through the stages, your recovery phase extends proportionally.
The following table depicts a summary of clinical observations. Each number represents a unit in time, usually day(s).
| Adrenal Fatigue Stage | Average Days of Adrenal Crash | Average Days it Takes to Recover | Ave. Total Cycle Time | Average Recovery Factor | Crash Time as % of Total Cycle | Recovery Time as % of Total Cycle | Recovery Factor Range |
|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 2 | 1 | 50 | 50 | 1 to 2 |
| 2 | 1.35 | 2.5 | 4 | 2 | 33 | 66 | 1 to 3 |
| 3A | 2 | 5 | 8 | 3 | 25 | 75 | 2 to 6 |
| 3B | 2 | 8 | 10 | 4 | 20 | 80 | 3 to 7 |
| 3C | 2 | 14 | 16 | 7 | 13 | 87 | 4 to 10 |
| 3D | 2 | 24 | 26 | 12 | 8 | 92 | 6 to 30 |
The RF sees a sharp increase in stage 3C where we see the greatest decline in adrenal function. You will also note a 43% increase between stages 3B and 3C, and 33% increase from 3A to 3B. Those in stage 3D, however, will spend 92% in recovery with only 8% in the crash phase. Those in the advanced stages of the condition should thus try to avoid crashes.
The following graph shows the difference between a successful and failed recovery program.
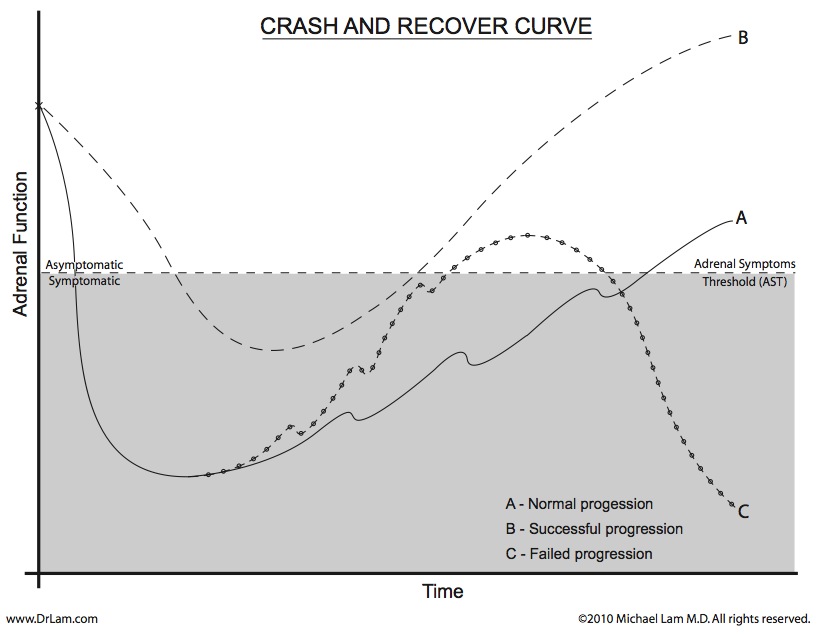
Line A shows a normal crash of average intensity followed by a typical prolonged recovery time common in Adrenal Fatigue stage 3C. It shows frequent setbacks during a slow, steady recovery.
Line B shows the same crash but under optimal recovery conditions. Such a recovery program does not guarantee a total absence of a crash. Intermittent crashes are unavoidable. A successful program, usually under experienced professional guidance, allows the sufferer a learning experience on how to recognize a crash before it comes and, when a crash occurs, the ability to use the necessary tools to slow down and lower the crash intensity. The goal is a crash that does not severely increase symptoms. It may also lessen your risk of a further crash.
A successful program will allow for a faster recovery phase and shorter total cycle time.
Line C represents a failed program. Most self-navigation programs fall into this category, especially for those with advanced Adrenal Fatigue or with a weak constitution. Recovery may seemingly progress well after a crash due to the use of stimulants like medications, herbs or glandulars. These fail because they cannot sustain adrenal function when your adrenals need careful nurturing. Symptoms may return and sometimes become worse. This could result in a more severe second crash resulting in a lower state of adrenal function. If this happens repeatedly, your body could move into the latter stages of adrenal fatigue that a good recovery program could have prohibited.
Knowing what to supplement with and when can become overwhelming. As a result, we started using our expertise in the field to simplify things for you. Furthermore, normal supplements do not always do what you expect them to. As a result, we at Dr. Lam have created our own line of supplements based on our experience and research. When dealing with the adrenal crash and recovery cycle, we suggest the following:
 FermPlex A: A blend of fermented herbs that include ashwagandha, Holy basil, peppermint, and ginseng. Together, these herbs may help improve the various symptoms associated with adrenal fatigue and help in overcoming crashes.Recommended dosage: 1-4 servings per day.
FermPlex A: A blend of fermented herbs that include ashwagandha, Holy basil, peppermint, and ginseng. Together, these herbs may help improve the various symptoms associated with adrenal fatigue and help in overcoming crashes.Recommended dosage: 1-4 servings per day.Please note that we highly recommend your first talk to an experienced provider before taking any supplements. They are best able to determine their efficacy and dosage. Furthermore, please remember that certain supplements may interfere with medications or impact underlying health conditions.
Managing an adrenal crash proves both difficult and perplexing. This is because those with the condition go through adrenal crash and recovery cycles. These cycles haunt sufferers until adrenal function becomes normal once more.
Unfortunately, self navigation or going to a healthcare provider not conversant with the condition may both contribute to recovery failure. A healthcare provider cognisant of the condition will employ a detailed investigation and examination to find the cause of each crash to better help in your treatment procedure.
If you would like to know more about how to heal your adrenal fatigue and crash and recovery cycles, the team at Dr. Lam Coaching can help. We offer a free** no-obligation phone consultation where we will privately discuss your symptoms and current treatment protocols. You can also contact us via our Ask The Doctor system by clicking here.
"12 Leading Causes of Death in the United States." 12 Leading Causes of Death in the United States, www.healthline.com/health/leading-causes-of-death.
Kelly C;Jefferies C;Cryan. “Targeted Liposomal Drug Delivery to Monocytes and Macrophages.” Journal of Drug Delivery, pubmed.ncbi.nlm.nih.gov/21512579/. Accessed 8 May 2023.
Kameda, Kin-ya, and Yasushi Abiko. "Stimulation of Fatty Acid Metabolism by Panteth(E)Ine." Stimulation of Fatty Acid Metabolism by Panteth(E)Ine | SpringerLink, https://doi.org/10.1007/978-1-4613-3045-5_40.
BCP are designed to regulate menstrual flow. Advanced sufferers of AFS can find hormonal rebalancing destabilizing which can trigger an adrenal crash. This is not common, however.
Any crash is not healthy for the mother and the fetus because it requires the body to expand its resources for recovery which would drain the existing resources. Remember there are no good crashes. Therefore it is imperative for those who are pregnant to take good rest and nurture the body as much as possible.